
Breathwork for Posture and Strength
Low back pain is classified as the leading cause of disability globally — at 7.4% across all age groups, and 5.4% among working adults.¹ ² Most cases are classified as "non-specific," meaning no single structural pathology or underlying issue has been identified.²
Research has also repeatedly reported that over 50% of people with chronic lower back pain also show dysfunctional breathing patterns.³ ⁴ Even higher percentages of dysfunctional breathing are suggested to correlate with occasional or sporadic reports of back issues and pain — especially where anxiety and stress alter breathing patterns and manifest as tension or pain.⁵ ⁶
The Body as One Connected System
As practitioners, we see the body as one connected system. Considering a human being from more than one perspective — biological, psychological, and social — forms the basis. We therefore deem a person's habits, daily patterns that stimulate the nervous system, social environment, and psychological health just as important to physical health and wellbeing as direct movement and/or (strength) training.
When we breathe functionally, it can positively impact all of these areas. Besides that, our breathing pattern has a direct effect on posture, and on the body's ability to generate tension or physically relax.The stability of our core, the weight-bearing capacity of the spine, the symmetry of our skeletal system, and the tone of the facial muscles are all closely linked to the rhythm and quality of our breathing pattern — alongside the various benefits to our general health, mental and emotional wellbeing that we discuss in our keur teacher training and blog posts.
Safety as a Foundation for Posture and Strength
Recent advances in neuroscience place the brain as the central regulator of postural stability, mobility, and tension.The relationship is direct: when the brain can distinguish real threats from insignificant ones, movement is free. When threat-perception is high, movement becomes restricted — and the brain can even signal pain regardless of whether tissue damage is present.⁷ This makes having a sense of safety one of the most vital processes underlying healthy posture.
Functional breathing exercises, combined with graded movement exposure, can shift this balance. General mobility, aches, and back pain all correlate strongly with the body's moment-to-moment sense of safety. Breathing may be the most accessible tool we have for influencing it.
Biomechanical Anatomy of Breathing
The lumbar spine is positioned between the upper back (thoracic spine) and the hip (pelvic; sacral spine). When hip mobility is restricted, the body usually compensates through excessive lower back (lumbar) movement.⁸ ⁹
Why might this be relevant to breathing? The diaphragm is a primary muscle for respiratory function. Along with many interwoven groups of smaller muscles, it works as a kind of three-dimensional pump that supports the lungs to fully inflate and deflate. When any part of that movement is restricted, shortened, or misaligned — through instances such as hip restrictions, postural asymmetries/imbalances — the breath can become impaired.
There is a direct biomechanical pathway between the position of your spine and the quality of your breath. When the diaphragm cannot ascend and descend freely, breathing tends to become shallower and/or rapid; in risk of becoming dysfunctional. You might recognise this, shoulders and head tilted forward, rounded spine, and long hours of maintaining this position at a desk.
Pelvic Position and the Zone of Apposition
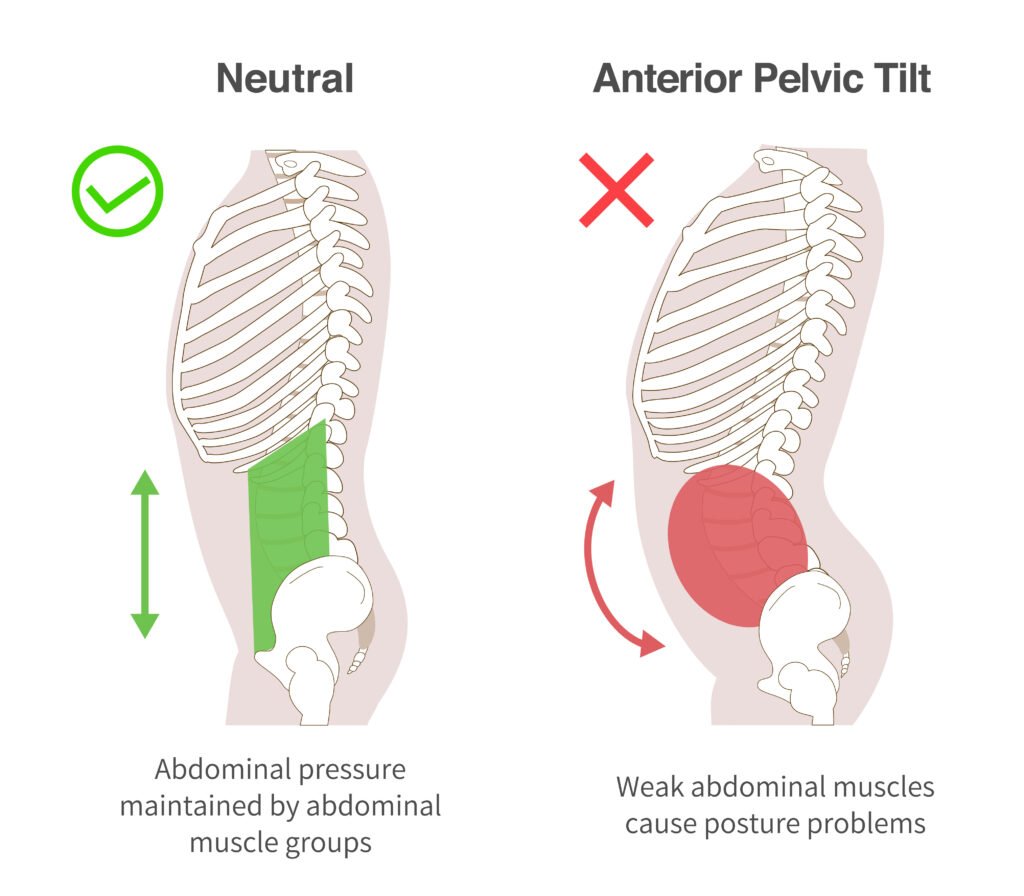
Image Source: Advanced Orthopedics and Sports Medicine Institute
Pelvic positioning can influence spinal alignment as well as respiratory function.
The frontal axis of the body — which includes the posterior and anterior pelvic tilt (the rotation of the hip from arch to round). This axis sets the diaphragm up for its ability to support a stable spine, as well as for optimal respiratory function through a full range of biomechanical motion. ¹⁵ ¹⁶
Tilting the pelvis into its optimal neutral position alters the available room that the lungs have to expand into and contract out of. This is called the zone of apposition. ¹⁷ With a full breath we mean not only the amount of air that goes into the lungs on the inhale, but also the parts of the lungs — lobes and volume of the alveoli — that are being used for gas exchange.
Hodges demonstrated that the intra-abdominal pressure (IAP) generated by the diaphragm directly stiffens the lumbar spine¹⁸ — meaning that pelvic tilt alters intra-abdominal pressure (IAP) dynamics, which in turn alters spinal stability, which in turn alters breathing strategy. Madle, Kolar et al. (2022) confirmed that DNS positioning protocols increase abdominal wall tension in postures that restore diaphragm–pelvic floor coordination: different postural positions produce different stabilisation patterns.¹⁴ Szczygieł et al. (2018) quantified that deep muscle training improves both postural alignment and breathing quality simultaneously.¹⁹
The practical implication for movement and strength training: before someone learns to squat heavy, deadlift, or press overhead, they must learn to breathe into a bracing hold. Not hold their breath against a closed throat — but create genuine 360° intra-abdominal pressure through coordinated diaphragmatic descent. This is a skill which can be practiced safely at any age under the right intensity level.
Intra-Abdominal Pressure and Strength
Kolar and the Prague School of Rehabilitation have spent decades studying how infants naturally generate intra-abdominal pressure (IAP) — they're born knowing how to safely move their spine and even brace. Watch a baby lift its head from a lying position and you'll see perfect 360° expansion of their belly, back, and sides of the body. Adults sometimes lose this ability through years of sitting, stress, and compensatory breathing.
Kolar et al. (2012) published landmark research showing that athletes with low back pain consistently demonstrated poor diaphragmatic function and inadequate ability to produce supportive intra-abdominal pressure (IAP)— even when their "core strength" (measured by planks, sit-ups, etc.) was normal.¹⁰ The problem wasn't strength. It was often a lack of coordination: proper timing and sequencing of breath and bracing patterns.
The diaphragm is both the primary respiratory muscle and a postural stabiliser. Another researcher (Hodges) demonstrated that diaphragm activation precedes limb movement — it establishes intra-abdominal pressure before the body moves.¹¹ ¹² When breathing is dysfunctional (chest-dominant, rapid, shallow), this stabilising role is compromised, and the lumbar spine bears more of the load or force. When breathing demand rises, the diaphragm sacrifices its postural function — meaning that if pelvic alignment is already poor, the system fails faster under load.¹³ Kolar built a clinical framework from developmental kinesiology — Dynamic Neuromuscular Stabilisation (DNS) — restoring diaphragm–pelvic floor coordination as the foundation of core stability.¹⁴
What functional intra-abdominal pressure looks like:
Inhale: the diaphragm descends fully; the belly, sides, and lower back expand simultaneously (360° expansion — not just the front)
The pelvic floorgently descends (it doesn't grip; it yields)
Before the lift: slightly inhale to fill the cylinder, then stiffen the wall — a gentle bearing-down pressure, like fogging a mirror with an open glottis
The trunk is now a pressurised column — the spine is protected by hydraulic force, not just muscular gripping
Note. From postural research: having proper control over the hip, proper activation of the glute muscles, and an ability to freely extend the hip, has been demonstrated to prepare the body most optimally for proper biomechanical breathing patterns and functional intra-abdominal pressure (IAP).⁸ ⁹
What dysfunctional intra-abdominal pressure (IAP)looks like:
Chest rises, belly sucks in (inverted breathing pattern)
Only the front of the belly expands (no lateral or posterior expansion)
Pelvic floor grips up and in (prevents diaphragmatic descent)
Holding the breath by closing /tension the This only increases intrathoracic pressure, which raises blood pressure and compresses cervical discs without stabilising the lumbar spine
An easy way to put this all into practice is by doing a breathing exercise that starts on the floor, and then we can build it up from there.
How to practice
1. Floor Breathing
Position: Lie face down. Forehead on stacked hands. Legs relaxed, toes pointed out.
Practice:
Inhale through the nose. Direct the breath into the belly against the floor. You should feel your abdomen push into the ground — front, sides, and lower back expanding.
Exhale slowly through the nose or gently pursed lips.
Time: Repeat for 2–3 minutes.
2. 90/90 Supine Breathing (IAP Training)
Position: Lie on your back. Feet on a wall (or chair), hips and knees both at 90 degrees. Low back gently flattened to the floor (posterior tilt of the pelvis).
Practice:
Inhale through the nose for 4 counts, feeling the ribs expand laterally (place hands on lower ribs to feel them).
Exhale through gently pursed lips for 8 counts, feeling the ribs compress inward and downward.
At the end of each exhale, pause 3 to 4 seconds. Notice the abdominal wall gently engaging.
Time: Repeat for 5 breaths. Rest. Then repeat for 3 rounds.
3. Slow Nasal Walk
Position: Dynamic, while walking.
Practice: Walk with your mouth closed, breathing only through the nose, and trying to maintain a neutral hip position and spine. Naturally, your pace will be limited by your nasal breathing capacity — if you can't maintain nasal breathing, slow down and continue for the duration of your walk. Try to breathe into all directions: 360°, and if you have a light elastic band, you can place it around your ribcage to feel the movement of your breath.
Time: 10-20 Minutes
Conclusion
The research is becoming clearer, and so is the clinical understanding: the way we breathe can shape how we hold ourselves, how we stabilise our spine, and how we access the strength our body is built for.
If you feel drawn, begin simply. Choose one of the exercises, perhaps starting on the floor. Breathe into the belly and notice the quiet expansion of your breath into the ground, into the sides of the body, into the back.
Find your access to the breathing muscles in all directions — 360°.
Sometimes, the way back to strength is not to push harder, but to listen more closely.
References:
GBD 2021 Low Back Pain Collaborators. "Global, regional, and national burden of low back pain, 1990–2020." The Lancet Rheumatology. 2023.
Vlaeyen JWS, Maher CG, Wiech K, et al. "Low back pain." Nat Rev Dis Primers. 2018;4(1):52.
Roussel N, Nijs J, Truijen S, Smeuninx L, Stassijns G, Stassijns G. "Low back pain: clinimetric properties of the Trendelenburg test, active straight leg raise test, and breathing pattern during active straight leg raising." Eur Spine J. 2007;16(5):S209–S214.
Smith MD, Russell A, Hodges PW. "Disorders of breathing and continence have a stronger association with back pain than obesity and physical activity." Aust J Physiother. 2006;52(1):11–16.
Garssen B, de Ruiter C, Van Dyck R. "Breathing retraining: a rational placebo?" Clin Psychol Rev. 1992;12(2):141–153.
Courtney R. "The functions of breathing and its dysfunctions and their relationship to breathing therapy." Int J Osteopath Med. 2009;12(3):78–85.
Butler DS, Moseley GL. Explain Pain. Adelaide: Noigroup Publications; 2003. See also: Brumagne S, Cordo P, Lysens R, Verschueren S, Swinnen S. "The role of paraspinal muscle spindles in lumbosacral position sense in individuals with and without low back pain." Spine. 2000;25(8):989–994.
Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. "The sacroiliac joint: an overview of its anatomy, function and potential clinical implications." J Anat. 2012;221(6):537–567.
McGill SM. Ultimate Back Fitness and Performance. 5th ed. Waterloo: Backfitpro; 2014.
Kolar P, Sulc J, Kyncl M, Sanda J, Cakrt O, Andel R, Kumagai K, Kobesova A. "Postural function of the diaphragm in persons with and without chronic low back pain." J Orthop Sports Phys Ther. 2012;42(4):352–362. PMID 22236693.
Hodges PW, Butler JE, McKenzie DK, Gandevia SC. "Contraction of the human diaphragm during rapid postural adjustments." J Physiol. 1997;505(Pt 2):539–548. PMID 9423192.
Hodges PW, Gandevia SC. "Activation of the human diaphragm during a repetitive postural task." J Physiol. 2000;522(Pt 1):165–175. PMID 10618161.
Hodges PW, Heijnen I, Gandevia SC. "Postural activity of the diaphragm is reduced in humans when respiratory demand increases." J Physiol. 2001;537(Pt 3):999–1008. PMID 11744772.
Madle K, Svoboda P, Stribrny M, Novak J, Kolar P, Busch A, Kobesova A, Bitnar P. "Abdominal wall tension increases using Dynamic Neuromuscular Stabilization principles in different postural positions." Musculoskelet Sci Pract. 2022;62:102655. PMID 35998419.
Aramaki Y, Kakizaki F, Kawata S, Omotehara T, Itoh M. "Effects of the posterior pelvic tilt sitting posture on thoracic morphology and respiratory function." J Phys Ther Sci. 2021;33(2):118–124. PMID 33642685.
Ishizuka T, Nishida N, Homma Y, Hirayama T, Ishida Y, Kakizaki F, Konishi M. "Instantaneous changes in respiratory function induced by passive pelvic suspension in the supine position in relation to increased diaphragm excursion." J Phys Ther Sci. 2017;29(3):432–437. PMID 28356625.
Boyle KL, Olinick J, Lewis C. "The value of blowing up a balloon." N Am J Sports Phys Ther. 2010;5(3):179–188. PMID 21589673.
Hodges PW, Eriksson AE, Shirley D, Gandevia SC. "Intra-abdominal pressure increases stiffness of the lumbar spine." J Biomech. 2005;38(9):1873–1880. PMID 16023475.
Szczygieł E, Blaut J, Zielonka-Pycka K, et al. "The Impact of Deep Muscle Training on the Quality of Posture and Breathing." J Mot Behav. 2018;50(2):219–227. PMID 28820662.